Guidelines developed from gallbladder patient data and interviews form the basis of a new effort to right-size opioid prescribing for many operations.
11:00 AM
Author |
Some surgeons might be able to prescribe a third of opioid painkiller pills that they currently give patients and not affect their level of post-surgery pain control, a new study suggests.
MORE FROM THE LAB: Subscribe to our weekly newsletter
That would mean far fewer opioids left over to feed the ongoing national crisis of misuse, addiction and overdose.
The findings, published in JAMA Surgery by a team from the University of Michigan, show the power of basing surgery-related pain prescriptions on how patients actually use medicines, and educating both surgical teams and patients on pain control. The U-M team recently launched a site aimed at doing just that.
Evidence-based guidelines
Because no national guidelines exist for surgery-related pain control with opioids, the team set out to develop some and test them. They started with a common operation: gallbladder removal, or laparoscopic cholecystectomy.
Data from 170 patients treated at Michigan Medicine, U-M's academic medical center, showed the average patient received a prescription of 250 milligrams of opioid medications, as measured in morphine equivalents. That's about 50 pills.
But when the researchers interviewed 100 of these patients, the amount of opioid painkiller they'd actually taken after the operation averaged 30 milligrams, or about six pills. The rest was often still sitting in their medicine cabinets, even years after surgery.
Immediate effect
When U-M surgical leaders heard these findings, they gave the researchers the green light to develop and roll out a much lower prescribing guideline, paired with a new patient education effort about pain control.
The result: At Michigan Medicine, the average prescription for gallbladder surgery patients dropped 66 percent, to 75 milligrams of opioids, or 15 pills, in the 200 patients treated in the first five months after the guideline went into effect.
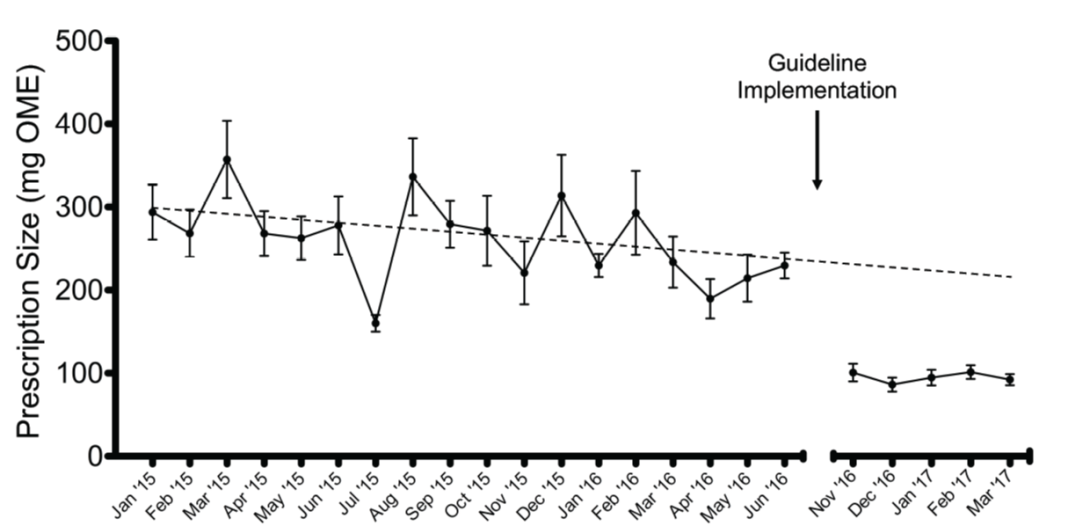
The percentage of patients getting a prescription for nonopioid painkillers such as acetaminophen or ibuprofen more than doubled. And requests for opioid refills didn't increase, as some clinicians feared.
Interviews with 86 of the patients who received the smaller prescriptions showed they reported the same level of pain control as those treated before — even though they took even less of their opioid medicine, about 20 milligrams.
"For a long time, there has been no rhyme or reason to surgical opioid prescribing, compared with all the other efforts that have been made to improve surgical care," says first author Ryan Howard, M.D., a resident in the U-M Department of Surgery who began the study while attending the U-M Medical School. "We've been overprescribing because no one had ever really asked what's the right amount. We knew we could do better."
SEE ALSO: Opioid Prescribing Recommendations for Surgery
He estimates that just implementing the guidelines for gallbladder surgery at U-M has kept more than 13,000 excess opioid pills out of circulation in the year since the rollout began.
We continue to notice that with education and attentive care, fewer and fewer opioids are needed and pain care is improving.Michael Englesbe, M.D.
Getting buy-in
The team stayed on the conservative side with the initial guideline, recommending 15 opioid pills for gallbladder patients.
Howard worked with fellow resident Jay Lee, M.D., and transplant surgeon Michael Englesbe, M.D., to perform the study and implement the guideline. Armed with the data and interviews from previous patients, they worked with surgical leaders, then met with nurses, physician assistants, residents and surgeons in turn.
"Even though the guidelines were a radical departure from their current practice, attending surgeons and residents really embraced them," says Lee. "It was very rewarding to see how effective these guidelines were in reducing excess opioid prescribing."
The team also used the insights gained from patient interviews to redesign patient education materials. For instance, some patients had said they had taken every opioid pill their surgeon had prescribed because they thought they were supposed to — like a course of antibiotics.
The new patient education guide for gallbladder removal counsels patients to take pain medicines only as long as they have pain, and to reserve the opioid pills for pain that is not controlled by ibuprofen or acetaminophen.
Many patients interviewed before the guidelines took effect said they wanted to know how many pills to expect to take, so the guide laid it out: Most patients take about five or fewer, and they stop taking pain medicine by the fifth day after surgery.
The guide also emphasizes the need for safe disposal of leftover pills, and it gives a link to a map created by the team showing locations across Michigan that take opioids back.
Based on the results, the team decided to take the guideline effort statewide and increase the number of operations. Using data from patients who had surgery at dozens of Michigan hospitals taking part in the Michigan Surgical Quality Collaborative, the team has developed prescribing recommendations for 11 common operations.
Less than two months ago, those recommendations made their public debut via the Michigan Opioid Prescribing and Engagement Network (Michigan-OPEN) initiative that Englesbe co-leads. The team notes that surgeons have mostly welcomed the recommendations as an evidence-based foundation for prescribing post-surgery pain medicine.
"Pain is an integral part of surgery — we cause pain in the short term so in the long term we can help heal you," says Howard. "Nearly half of the prescriptions surgeons write are for pain medications, but traditionally we haven't gotten any training or guidance in it. We hope that this framework we've developed can be applied to many more operations."
Building on previous work
The Michigan-OPEN team previously found that about 6 percent of surgery patients who receive opioids keep refilling their prescriptions months later — long after their pain should be gone.
The team also has published findings based on statewide data that show that patient satisfaction scores related to pain aren't linked to the amount of opioids prescribed. The worry that denying patients opioids will decrease satisfaction — and with it the extra payment that hospitals get from Medicare based on satisfaction scores — has been a constant refrain to the U-M team from surgical professionals.
Englesbe, a professor in the U-M Department of Surgery, is aiming even lower when it comes to opioids. "We continue to notice that with education and attentive care, fewer and fewer opioids are needed and pain care is improving," he says. "Our ambitious goals include empowering half of the surgical patients at Michigan Medicine to be opioid-free following the first day of surgery."

Explore a variety of healthcare news & stories by visiting the Health Lab home page for more articles.

Department of Communication at Michigan Medicine
Want top health & research news weekly? Sign up for Health Lab’s newsletters today!





